Survival in Adverse Conditions (2001)
An organized collection of photographs and quotations selected from studies finding evidence of alternate forms of various spirochetes, dating from the early 1900's through the present. Written permission to publish this article in LymeRICK from the author, who wants to remain anonymous.
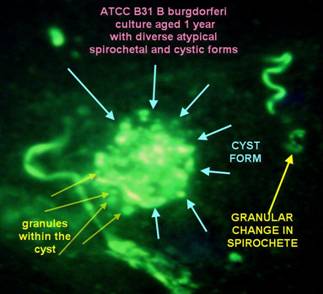
Culture of Borrelia burgdorferi (B31)
- stained with fluorescin marked specific anti-Borrelia antibody;
done circa 1985
Visit dr. MacDonalds new website on Alzheimer & Molecular biology / Borrelia
“Of Course you have my permission to include any of my images on your web site.
I Do not desire to copyright the images, because so many in the Lyme Borreliosis community have viewed these images over the 20 years since they were created, that it constitutes a de facto acknowledgment and I know that my photomicrographs exist to serve as tools for education, and not for commercial purpose.
The image of the "cystic" form was obtained from very aged cultures of B31 from the ATCC. After the motility of the borreliae ceased, the "formes atypiqes" appear, and there forms are very diverse. Cystic forms which contain granules inside of the cysts are just one of a
myriad of atypical forms that Bb may assume.”
[wrote Alan MacDonald to Marie Kroun in personal e-mail about this picture on 20050830]
Matti Viljanen, MD, Professor – Finland

Tube phagocytosis of Borrelia burgdorferi
(fast Internet connection Real Player Movie 3 Mb.
Above links to – and following is the text copied from –Viljanens own website:
”The video is a digitized version of the original video, from which the still images in figure 2 of the article "Tube Phagocytosis, a Novel Way for Neutrophils To Phagocytize Borrelia burgdorferi" by Juha Suhonen, Kaija T. Hartiala and Matti K. Viljanen (Infection and Immunity, July 1998, Vol. 66, No. 7) were captured.
The video is presented with the kind permission of American Society for Microbiology. The video presents a novel type of phagocytosis described in the article mentioned above. The original video was produced by observing and recording the interactions between human neutrophils and Borrelia burgdorferi, the Lyme disease spirochete, using dark-field microscopy with video technology. The digital version was made by Antero Lehtonen.”
 0018-GCS2.wmv 18 MB, 2 minutes video first presented at the conference in York 2003 in this PowerPoint lecture
0018-GCS2.wmv 18 MB, 2 minutes video first presented at the conference in York 2003 in this PowerPoint lecture
Microscopy of unfixed, unstained wet drop of peripheral blood from MKs pilot project patient #18
Case history was presented in MKs lecture in York, UK, 2004, presenting as leucocytoclastic vasculitis which has been found associated with Borrelia infection in a few cases!
This patient was first diagnosed with Borrelia burgdorferi plus tick borne co-infections with HME and Babesia like organisms back in December 2001!
This video is from April 2003, i.e. about 16 months after the initial diagnosis and despite intermittent antibiotic treatment with doxycyclin for a few months, and demonstrates a “pearls on a string” spirochete like structure that can be seen moving inside a cellular structure, possibly a white blood cell?
Despite bad video quality, it should be obvious to everyone seeing this video, that it is NOT a NORMAL finding within a white blood cell to find a structure moving serpentine like - as illustrated in this video!

Since 2005 MKs videos has improved considerably, after she got a new handy video camera for USB – a Bresser PC-Microocular-II (cost only 99.95 Euro), which fits into the ocular of most microscopes.
A newer video of BUFFY-COAT fraction of blood of the same patient (#18) as above was taken 4 years after first diagnosis – 0018-20051213.wmv – shows persistence of similar blood changes compatible with persistent Borrelia infection, despite more oral courses of antibiotic treatment in between, leading to only temporary improvement in his clinical condition. Though obvious signs of vasculitis are rarely present nowadays – he still gets a few petecchiae now and then during his worst flares – he has many other fluctuating symptoms consistent with chronic Borreliosis, i.e. a chronic fatigue syndrome / ME-CFS like symptom presentation, like most other chronic Borreliosis project patients display!
A RECENT VIDEO taken by MK with this camera was done on a fresh BUFFY-COAT wet blood drop (WMV, 50 Mb, 6 minutes): 0049-20060704.wmv – illustrates spirochetes and granules.
Same pt. after 3 months treatment (WMV, 165 Mb incl. above movie): 0049-20061024.wmv
Samples were taken the day after start of symptom flare on a male patient, who was diagnosed in Jan. 2006 with brain infarct and certain neuro-Borreliosis, i.e. by being spinal antibody index positive for Borrelia burgdorferi and by having increased number of white blood cells in his spinal fluid, and who had improved a lot, but only temporarily, on the usual two-week treatment with intravenous ceftriaxon; he relapsed within a few months after stopping antibiotic treatment, was denied re-treatment because his neurologist thought he had been cured of Borreliosis because his Borrelia antibody response dropped after treatment! – after above confirmation of his relapse of active Borreliosis, he has started oral antibiotic re-treatment, has experienced a Jarisch-Herxheimer reaction within the first week of treatment and begin to feel improvement again, thus so far he follows the usual treatment pattern for chronic Borreliosis.
So far (July 06) 48/48 patients (#42 was reserved, but has not been Bowen tested yet) with similar structures found in their blood by microscopy and displaying current symptoms compatible with having active Borreliosis, had positive outcome of a specific immune stain for Borrelia burgdorferi, done by Bowen RTI, see below!
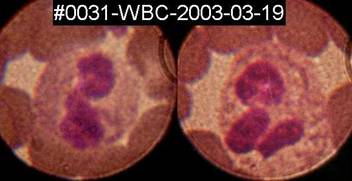 Spirochete like structures can sometimes, but rarely, be seen inside white blood cells, here inside two granulocytes on a fixed, Diff-Quik stained blood-smear from patient#31.
Spirochete like structures can sometimes, but rarely, be seen inside white blood cells, here inside two granulocytes on a fixed, Diff-Quik stained blood-smear from patient#31.
Thus Marie Kroun’s microscopy findings support the observation done by others, that Borrelia burgdorferi can be located inside WBC and possibly also RBC, since not all the cellular structures with moving granules in it contain a visible nucleus!
While it seems that any type of white blood cell – neutrophile, eosinophile (and possibly also basophile?) granulocytes, as well as monocytes and lymphocytes judging from the appearance of the nucleus, can apparently harbour moving “granules” of spirochetes, it is also obvious to MK that it is not all “granulated cellullar structures” that contain a nucleus!
Note that monocytes and lymphocytes, which have either a kidney shaped or a round nucleus without lobes, does not normally contain any granula in their cytoplasm, so when moving i.e. alive “granules” are found within the “mononuclear” cell types, there is NO possible confusion about what is normal / abnormal “granules”, its clearly abnormal when found in mononuclears!
More important, the spirochetal “granules” are usually larger and also a bit darker in appearance in phase contrast microscopy, than the normal granula found within the cytoplasm of the normal granulocytes, and last but not least granula within a normal granulocyte do NEVER move in a “pearls on a string” / spirochete like fashion!
Thus Borrelia – this master of disguise microbe – probably can use a wide variety of host cells as a sheltered environment during its development, just like we will shelter a newborn, weak baby in an incubator. This is very far from being a NEW OBSERVATION!
Already Balfour in Lancet 1911 described that granules of fowl spirochetes entered RED BLOOD CELLS and Hindle in 1912 drew spirochetes and granules inside nucleated cells found within the Argas tick!
Unstained wet-drop microscopy can be done on a fresh ear prick blood sample, on anti-coagulated full blood (EDTA, citrate) or maybe even best on sample from the Buffy-Coat fraction — see MKs how to make buffy-coat smear video – because as shown by MKs video samples from buffy-coat wet drop preparation, it appears to be ideal for finding (moving) “granulated cellular structures” and could be combined with use of a highly specific immune stain for any suspected pathogen, for more specific diagnostics, like done by Bowen RTI, however, quantification does not make any sense on buffy-coat fraction, of course!
Moreover, the buffy-coat fraction is ideal material for finding many other blood parasites, since both free microbes and immune cells, that have phagocytised microbes, fulfilling their normal task of trying to eliminate foreign intruders from the blood, will concentrate in the buffy-coat fraction, see some references on buffy-coat microscopy for parasites: QBC Malaria, Paralens, and Google and PubMed search.
While wet blood drop preparation is short-lived because the blood cells lyses within a few days or hours, if contact with air is not avoided by packing the edge of the cover glass for instance with Vaseline (avoid contamination of the blood sample when applying), the buffy-coat blood smears can be stored for several years ahead for later examination!
A German colleague and good friend, who is a tropical disease specialist, gave MK a 20-year old blood smear from a malaria patient; we stained it and looked in the microscope and really couldn’t tell that it wasn’t a recent smear; malaria parasites were easily visible in it, many more than is usually the case with the tick-borne cousin babesia!
Since the cost of the glass slides are low, they don’t take up much space if you stack them in the same box you bought the slides in, and the smears can later be used for trying other stains for comparison, for using additional (more specific immune) stain or you might even scrape blood off the slide for doing PCR test in order to get a more specific diagnosis than just “ringforms seen” or “morulae-like inclusions seen”, or you might use it for education of laboratory workers and colleague microscopists etc. – THEREFORE ALWAYS TAKE PLENTY (buffy-coat) BLOOD SMEARS whenever you have the chance; you can really never get too many good blood smears with parasites in it, and you may have only ONE chance per patient before treatment to catch some of these parasites of which there are usually few in relatively few of the chronically ill patients with tick borne infections!

Dr. Joanne Whitaker et al. patented their procedure for detecting Borrelia burgdorferi ANTIGEN by specific fluorescent antibody stain in Jan. 2005, see the US-patent (6,838,247) for all details about their Q-RIBb method!
The main advantages of Bowen RTIs Q-RIBb test are:
1. Documentation by picture(s) of any microscopic finding, so you can compare your own microscopy findings to that
2. Quantifying - by titration - the number of structures reacting with added specific antibody against Borrelia burgdorferi.
As stated in the patent description Bowen RTI use a commercially available FITC-labelled anti-Borrelia burgdorferi antibody from Kirkegaard & Perry Lab.:
Affinity purified polyclonal antibody to Borrelia burgdorferi made in Goat and labeled with fluorescein isothiocyanate (FITC). Isolated from a serum pool of goats immunized with heat killed whole cells of Borrelia burgdorferi. The antibody is highly specific for Borrelia burgdorferi. Cross reactivity to Borrelia hermsii, Borrelia coriaceae, and Borrelia anserine has been minimized through extensive affinity adsorption. Product is in lyophilized form. Each lot is tested to assure specificity and lot-to-lot consistency using KPL's in-house ELISA assay.
 AndyWright2004-640.wmv (52 Mb, 4 minutes) video of spirochetes in more lenghts, granules, a moving granulated cellular structure, thus illustrating all the phases complex spirochetal lifecycle drawn on page 475 in this article by Hindle 1912 (PDF) printed in Parasitology (1912), iv, pp 463-477.
AndyWright2004-640.wmv (52 Mb, 4 minutes) video of spirochetes in more lenghts, granules, a moving granulated cellular structure, thus illustrating all the phases complex spirochetal lifecycle drawn on page 475 in this article by Hindle 1912 (PDF) printed in Parasitology (1912), iv, pp 463-477.
So far (June 2005) 98/98 of Andy’s ME/CFS patients with such structures in their blood tested positive on direct fluorescent antibody test for Borrelia burgdorferi ANTIGEN!
 Dualdur® movie
Dualdur® movie
70 Mb, 11 minutes dark-field microscopy video of Borrelia burgdorferi spirochetes in blood, showing the shedding of ‘granules’, budding of the spirochete at the end and centrally, the formation of blebs and transversal division of the spirochete. Dr. Bozsik adds a reagent to the blood named Dualdur, on which he holds the patent, which immobilizes blood cells, but do not disturb the spirochetal movements.
Dr. Bozsik kindly gave me his permission to present both his lectures - DIAGNOSIS and THERAPY – held at the Sheffield 2005, UK LDA conference on tick-borne infections
Both presentation are made in PowerPoint 2003; some embedded videos from “The Passion of Christ” and “biting tick” shown at the conference, does not seem to work properly from within in this PowerPoint presentation when online?
The latter - tick bite video - show us how an Ixodes tick enters its hypostoma (blood suction organ) directly into a small skin capillary.
The implication is that when the tick has Borrelia burgdorferi in its salivary glands – some 5% to as many as 35% of examined ticks have been reported to be “systemically infected” with Borrelia and these ticks already harbour spirochetes in their salivary glands and thus do NOT need about 24 hours for becoming infective – they might transmit Borrelia infection immediately when they bite, as the spirochetes will be injected directly into the blood-stream with the ticks saliva!
Thus we must all realize by simple logic that Borreliosis must always be a blood infection right from start, explaining how spirochetes can spread very early into all tissues and compartments, like the central nervous system within only two weeks of the tick bite – weeks before or without any development of concurrent ERYTHEMA MIGRANS which is NOT, as it is usually described, a PRE-NEUROBORRELIOSIS manifestation, but is to be considered a possible SIDE MANIFESTATION of Borreliosis, possibly already having spread hematogenously, which is fully consistent with the fact that a previous or simultaneous Erythema migrans is recorded in just about 50% of cases that present with neuro-Borreliosis!
The implication of recognizing the possibility of EARLY SPREAD is that any antibiotic treatment for Borreliosis should always aim to reach a sufficient concentration, i.e. over the minimal inhibitory / bactericidal (MIC/MBC) concentration, within the central nervous system (CNS) and other deep tissues, also for early Borrelia infection, i.e. also when “just” the telltale sign of Borreliosis: Erythema migrans is present!
– otherwise there is a potential risk that some slightly more antibiotic resistant Borrelia may have spread to and can survive in relative undertreatment within the CNS or in other deep tissue compartments, from which a later bout of active Borreliosis could come, that can be much harder to treat effectively, due to selection of more antibiotic resistant variants because they survived at suboptimal antibiotic concentration may need higher dosis next time in order to be effective!
Many published reports on cases of progression of symptoms / relapses of Borreliosis after early, but low dose and short time antibiotic treatment for erythema migrans (usually with tablet penicillin or low dose doxycyclin given for only 10-14 days), show us that this risk is not just a hypothetical concern!
Dr. Bozsik found – data extracted from his Diagnosis lecture– that:
MORE ABOUT SERONEGATIVE BORRELIOSIS:
A considerably high number of patients with proven late Borreliosis, i.e. where persistent Borrelia infection was proven by ANTIGEN DETECTION - either by CULTURE, PCR and/or MICROSCOPY (sometimes aided by specific immune stain) for Borrelia burgdorferi
- has unfortunately been shown to test SERONEGATIVE on a wide variety of BORRELIA SEROLOGY tests – as demonstrated for instance in the reports listed in the following section.
Oksi et al. J Clin Microbiology 1995 Sep; 33(9): 2260-4 (PDF):
· All 41 patients had symptoms of Borreliosis for at least 3 months i.e. were LATE Borreliosis cases.
78.0% were sick for >= 6 months, 53.7% were sick for over 1 year!
"…. multiple organs were frequently involved. Recurrent fever episodes were seen in nearly half of the patients, neurological symptoms were seen in more than half of the patients, and musculoskeletal manifestations were seen in three-fourths of the patients. Moreover, most of these manifestations were long-lived. In spite of this, several patients were seronegative and most seropositive patients had only weakly positive antibody levels.”
· All patients were positive for Borrelia burgdorferi ANTIGEN:
12 were positive on CULTURE, 39 were positive on PCR – 10 were positive on both CULTURE & PCR!
· Performance of 3 different SEROLOGY tests all used on all 41 patients:
… data from table 2, page 2261; however, MK added % calculation and text enhancements to the table:
Sensitivity (~ true positives in patients) and specificity (~ true negatives in controls) are marked with bold and black.
False positive (in controls) and false negative (in patients) are marked with bold and red.
|
|
SA-ELISA IgM, IgG, or both |
FL-ELISA IgM, IgG, or both |
P39-ELISA |
|||
|
|
Positive* |
Negative |
Positive* |
Negative |
Positive* |
Negative |
|
Culture positive (n=12) |
11 26.8% |
1 2.4% |
6 14.6% |
6 14.6% |
5 12.2% |
7 17.1% |
|
Only PCR positive (n=29) |
21 51.2% |
8 19.5% |
11 26.8% |
18 43.9% |
1 2.4% |
28 68.3% |
|
Total patients (n=41) |
32 78.0% |
9 22.0% |
17 41.5% |
24 58.5% |
6 14.6% |
35 85.4% |
|
Controls (n=37) |
4 10.8% |
33 89.2% |
5 13.5% |
32 86.5% |
2 5.4% |
35 94.6% |
* Positive results include weakly positive, positive as well as strong positive results!
Note that % of patients who had true positive serology with P39-ELISA was less than the chance of hitting 6 when throwing a dice (1/6 ~ 16.7%)!
· Overall results of ALL 3 SEROLOGY tests on ALL 41 patients:
Sensitivites (true positives) for combined tests:
SA-ELISA + FL-ELISA: 80.5%; SA-ILISA + P39-ELISA: 80.5%; FL-ELISA + p39-ELISA: 51.2%
SA-ELISA + FL-ELISA + p39-ELISA: 82.9% - thus for only 34 of 41 patients, the diagnosis could be confirmed by positive serology, thus
7 of 41 (17%) patients were SERONEGATIVE on ALL THREE serology test, despite having proven LATE Borrelia infection!
· Although ALL patients suffered from symptomatic LATE LYME BORRELIOSIS, 18 (43.9%) had ONLY positive Borrelia-IgM, i.e. were Borrelia-IgG negative, respectively 10 (24.4%) on SA-ELISA and 8 (19.5%) on FL-ELISA.
Both FL-ELISA and P39-ELISA detected only one positive specimen which had gone undetected by the other two tests.
Eldøen et al. Tidsskr Nor Lægeforen 2001; 121: 2008-11 (PDF in Norwegian):
· 14 of 25 (56 %) patients with spinal index positive (~certain) NEUROBORRELIOSIS had specific borrelia-IgM and IgG-antibodies ONLY in their spinal fluid, while their - at same time as spinal fluid sampled - SERUM samples were negative for Borrelia-antibodies.
The Norwegian laboratory used two different serology tests, one of which is the above mentioned FL-ELISA (DAKO)!
The 14 FALSE SERONEGATIVE patients would probably have gone undiagnosed and untreated for their certain neuro-Borreliosis, if their Norwegian doctors had relied ONLY on their false negative SERUM Borrelia antibody result as been a 100% reliable diagnostic measure to out-rule the possibility of neuro-borreliosis, as many doctors are unfortunately still in the habit of doing!
… HMMM when serology test overlooked over half of the truly very sick patients in their SERUM samples, how many patients could have been missed on false negative spinal fluid ELISA’s, perhaps another 50%? ..
Lomholt H et al. Acta Derm Venereol 2000 Sep-Oct;80(5):362-6 (PMID: 11200835 ):
· From PubMed abstract: “The kinetics of antibodies to Borrelia burgdorferi following successful treatment of early and late cutaneous borreliosis were analysed in consecutive serum samples by an enzyme-linked immunosorbent assay (ELISA) technique.” [Danish study, so it was probably FL-ELISA from DAKO, Glostrup!?]
“Twenty-three patients with culture positive erythema migrans were followed for 23+/-14 months: 41% stayed seronegative, 35% showed an isolated immunoglobulin M (IgM) response, 8% an isolated IgG response and 16% a combined IgM and IgG responses. …. In general, antibody levels peaked within the first 3 months of symptom onset, whereafter a gradual decline was observed within 1 year. Treatment success may in part be monitored serologically for both seropositive erythema migrans and chronic cutaneous borreliosis as most patients show declining titres after successful treatment. However, continuously high titres do not necessarily indicate treatment failure.”
Oksi et al. Ann Med 1999 Jun;31(3):225-32. (PMID: 10...)
· 32/165 = 19,4% had clinical relapse after more than 3 months antibiotic treatment for borreliosis.
· In 13/32 (40,6%) could the relapse be verified by either positive PCR (12) and/or positive culture (3) for B. burgdorferi
· At time of proven relapse 6/13 (46%) were seronegative!
· 12/13 were seropositive at initial diagnosis, i.e. 5 pts. developed seronegativity despite proven persistent borreliosis!
· 5/13 (38%) had circulating immunecomplexes, of these 3 were seronegative.
· 1 patient (10) was seronegative throughout the whole course of illness despite both positive culture and PCR in CSF primarily, and positive biopsy and plasma PCR for Borrelia burgdorferi at time of relapse!
This patient had been treated with ceftriaxone IV 2g for 3 weeks, followed by 24 weeks of doxycycline 100 g bid and amoxicillin 1 week - a total of 28 weeks (6-7 months).
· 1 patient (8) had been treated for as long as 47 weeks (11 months) including 7 weeks of intravenous ceftriaxone - primary diagnosis was confirmed by positive biopsy and the relapse 44 weeks after treatment confirmed by a positive plasma PCR for Bb.
· 1 patient (2) had relapse 130 weeks after 1. treatment, that had lasted 16 weeks. Pt. was seropositive initially (both IgM and IgG), but seronegative at time of relapse; the relapse was confirmed by positive PCR for Bb, no history of re-infection in the meantime.
Marie Kroun’s pilot-project on patients all highly suspect for chronic Borreliosis, presented at medical conferences in UK and PowerPoint presentations from 2003 and 2004 presented in LymeRICK website:
· 36% of 33 patients tested SERONEGATIVE on the danish serology test for Borreliosis (FL-ELISA, DAKO) despite all presented with abnormal structures in their blood, as shown in above videos, and similar structures were confirmed to be Borrelia burgdorferi related, by positive stain in Bowen RTIs (Q-) RIBb test for Borrelia burgdorferi!
… more follows from the long term follow-up project in due time
· It was a similar case as in the Norwegian study that started MKs special interest for Borreliosis back in 1994; a 9-year old boy that was highly suspect of Borreliosis due to severe burning pains in both his legs, but who tested SERUM negative for Borrelia antibodies more times, a factor leading to delayed spinal puncture, which, when finally done, showed SPINAL FLUID was HIGHLY Borrelia ANTIBODY positive by FL-ELISA, while at the same time sampled BLOOD SERUM was SERONEGATIVE and the boy was still SERUM ANTIBODY NEGATIVE for Borrelia 4 months later!
THESE AND MANY OTHER PUBLISHED WORKS ALL EMPHASISE THAT ANY NEGATIVE BORRELIA SEROLOGY TEST CAN NOT BE USED TO EXCLUDE PERSISTENT ACTIVE BORRELIOSIS in the SYMPTOMATIC PATIENT – not even when more SEROLOGY tests are being used in combination!
Thus a declne in antibody result after antibiotic treatment, SHOULD NOT be taken as a positive sign of the Borrelia infection was cured forever, especially not when the patients symptoms recur shortly!
– when symptoms reappear within less than 1-3 YEARS after stopping antibiotic treatment for proven Borrelia infection, then suspect a relapse of ACTIVE Borreliosis and seek proof of it by all possible means!
When suspecting RELAPSING or CHRONIC PERSISTENT ACTIVE BORRELIA INFECTION – forget using ANTIBODY tests as the first diagnostic measure!
… the only proper use for Borrelia serology is that it can sometimes help prove EARLY Borrelia infection, since a negative serology test sometimes but unfortunately not always turns positive a while into the Borrelia infection.
Serology is of NO PRACTICAL USE in LATE Borrelia infection, because
1. multiple serology test were FALSE negative in several culture, PCR and/or microscopy proven cases of highly symptomatic Borreliosis patients, that usually showed benefit from antibiotic treatment at least as long as it was being given! – and because
2. serology can persist positive for years in asymptomatic individuals with latent Borrelia infection, who won’t benefit from antibiotic treatment, unless their latent infection begin to show signs of renewed ACTIVITY, i.e. the patient becomes symptomatic again! … and because
3. serology results can sometimes be “false positive”, due to cross reaction with other bacteria with similar antigens
Hence serology bear both a very high risk of undertreatment and of overtreatment ..
PLEASE NOTE THAT UNDERTREATMENT of Borreliosis is MUCH WORSE for the patient than "OVERTREATMENT" of clinically suspected persistent Borreliosis, because the side effects of antibiotic treatment are usually neither severe nor longer lasting - while letting Borreliosis go on untreated can be debilitating and even deathly for the patient in question!
INSTEAD OF SEROLOGY DO FULL BLOOD MICROSCOPY (preferably of buffy-coat fraction), which any doctor with a microscope could quickly learn to do by looking at the video's on this website!
- and if found changes like shown in the video’s and pictures above, TRY TO CONFIRM BY SPECIFIC ANTIGEN TESTS, whenever possible!
It is important to try to confirm the clinical diagnosis with more ANTIGEN tests, because finding any positive ANTIGEN test (in opposition to a positive ANTIBODY test) helps justify trial treatment with antibiotics and also justify the need for social economic support, when the patient suffers from so many invalidating symptoms, documented in the patients symptom diary, that can prevent her/him from working for a long (sometimes life-long) period of time due to persistent ACTIVE Borreliosis!
Because all spirochetes seem to go through all the same changes during their developmental cycle, as demonstrated in Survival in Adverse Conditions (2001) – any spirochete would possibly give about the same microscopic picture … thus
it is important to understand that wet blood drop microscopy can NOT ALONE be used to diagnose Borrelia burgdorferi infection specifically; diagnosis made by wet blood drop microscopy as shown by MK can ONLY be “suggestive of spirochetosis”!
So should you ever happen to see similar (moving) “granulated cellular structures” as shown in the videos on this website, in an unstained wet blood drop microscopy or you see spirochete like structures situated within blood cells in a stained blood smear or see spirochete like structures moving in plasma (outside cells), then you should always do supplementary SPECIFIC ANTIGEN DIAGNOSTICS, like doing microscopy with specific immune stain for B. burgdorferi, PCR and/or try to culture the microbes for confirmation / typing of the spirochete!
IF the treating physicians would just CARE to follow and test these patients thoroughly for Borreliosis and co-infections with ANTIGEN tests, which is NOT DIFFICULT, as illustrated in this article! – and treat them for ACTIVE INFECTIONs, instead of mocking these patients by stating FALSELY that “all Borrelia was killed after 10-14 days”, and calling them “hypochondriacs”, I’m quite sure many cases of chronic Borreliosis, long term suffering and disability could be prevented!
Despite improved diagnostic methods, like by doing live video-microscopy / plus specific immune stain for Borrelia, in order to document the presence of spirochete(s) and/or their alternative forms, during all active stages of Borreliosis, the diagnosis of Late (chronic) Borreliosis remains – probably forever – a CLINICAL DIAGNOSIS, that can sometimes, but not always be SUPPORTED by any POSITIVE TEST RESULT, but can NOT BE OUT RULED by any NEGATIVE TEST RESULT! – so LISTEN to the patients, let them write SYMPTOM DIARY!